
Maryam Dehghankhalili, MD,* Soghra Fallahi, MD, Forugh Mahmudi, MD,Fariborz Ghaffarpasand, MD, Mohammad Esmaeil Shahrzad, MD, Mohsen Taghavi, MD, and Marjan Fereydooni Asl, MD
*Health Policy Research Center, Shiraz University of Medical Sciences, Shiraz, Iran; Research Center of Molecular Medicine, Hormozgan University of Medical Sciences, Bandar Abbas, Iran; Fertility and Infertility Research Center, Hormozgan University of Medical Sciences, Bandar Abbas, Iran; Neuroscience Research Center, Shiraz University of Medical Sciences, Shiraz, Iran; Student Research Committee, Hormozgan University of Medical Sciences, Bandar Abbas, Iran
A B S T R A C T
Introduction. Female genital mutilation/cutting (FGM/C), also known as female circumcision, is an ancient traditional procedure that involves partial or total removal of the female external genitalia for nonmedical reasons. Although it is well described in African and some Arabic countries, data from Iran are scarce.
Aim. To describe the epidemiology, regional characteristics, knowledge, and attitude toward FGM/C in Southern Iran.
Methods. This cross-sectional study was conducted during a 36-month period from 2010 to 2013 in Hormozgan, a southern province of Iran near the Persian Gulf. We included 780 women in six major rural areas of the province who referred to healthcare centers for vaccination, midwifery, or family planning services. All participants underwent complete pelvic examination to determine the type of FGM. The questionnaire consisted of several sections such as demographic and baseline characteristics, and two self-report sections addressing the knowledge and attitude toward FGM/C and its complications. Baseline sociodemographic characteristics including age, educational level, marital status, religion, and nationality were the independent variables.
Results. Among the participants, 535 (68.5%) had undergone FGM/C. FGM/C was associated with higher age (P = 0.002), Afghan nationality (P = 0.003), Sunni Islam as religion (P = 0.019), illiteracy (P < 0.001), and family history of FGM/C in mother (P < 0.001), sister (P < 0.001), and grandmother (P < 0.001). Ancient traditions in the area (57.1%) were mentioned as the most important factor leading to FMG/C. Urinary tract infection was the most common reported complication (60.4%).
Conclusion. FGM/C is a common practice in rural areas of Southern Iran. It is associated with increased age, illiteracy, Sunni Islam religion, Afghan nationality, and positive family history. Lack of knowledge toward FGM/C is the main cause of its high prevalence and continuation in the area. Dehghankhalili M, Fallahi S, Mahmudi F, Ghaffarpasand F, Shahrzad ME, Taghavi M, and Fereydooni Asl M. Epidemiology, regional characteristics, knowledge, and attitude toward female genital mutilation/cutting in Southern Iran. J Sex Med 2015;12:1577–1583.
Key Words: Female Genital Mutilation/Cutting; Female Circumcision; Knowledge and Attitude; Determinants; Iran
Introduction
Female genital mutilation/cutting (FGM/C), also known as female circumcision, is an ancient traditional procedure that involves partial or total removal of female external genitalia for nonmedical reasons [1,2]. According to the World Health Organization (WHO), there are four main types of FGM/C: type I (clitoridectomy), type II (excision), type III (infibulation or pharaonic circumcision), and type IV, which are used to describe all other harmful procedures to the female genitalia in the absence of medical necessity [3]. The nomenclature for the practice varies across regions, ideological perspectives, and research frames. We use the expression preferred by United Nation’s International Children’s Emergency Fund and United Nation’s Population Fund, the two central policymakers in the global effort to end the practice, “female genital mutilation/cutting” (FGM/C) [1]. Since the early 1970s, Western efforts to end FGM/C have relied primarily on two frames that have influenced the discourse of FGM/C and, in turn, the ideological contestation over the practice [4,5]. FGM/C has not only been associated with violation of human rights, but has also been shown to be associated with impaired physical and mental health [6,7]. Several physical and mental complications have been associated with FGM/C including pain, bleeding, localized infection and abscess formation, pelvic inflammatory disease (PID), sepsis, tetanus, urinary problems such as urinary tract infection (UTI), hepatitis and human immunode ficiency virus (HIV) infection, and reproductive problems. Psychiatric complications include post- traumatic stress disorder (PTSD), flashbacks to the event, and affective disorders [8–10].
FGM/C is a worldwide practice being mainly reported in African and Middle Eastern countries. It has been estimated that about 100 and 140 women and girls have experienced FGM/C [11]. FGM/C is currently practiced in more than 28 countries among different ethnic and religious groups. It is estimated that about 1.5 million girls undergo FGM/C annually [12]. Although the epidemiology has been evaluated in several countries, the predictive factors and social determinants remain unknown and undetermined. Such data would be helpful for understanding the variation in the frequency of FGM/C as well as trends for its performance despite the legislations. In addition, reports from Iran are scarce, and only few studies have addressed the issue, previously [13,14]. Accordingly, we performed the current study in order to estimate the prevalence of FGM/C and the knowledge and attitude of women toward it in Southern Iran. We also aimed to identify the correlates of these beliefs to identify high-risk subpopulations.
Materials and Methods
Study Population
This cross-sectional study was carried out in a 36-month period from September 2010 to September 2013 in Hormozgan, which is a Southern region near the Persian Gulf in Iran. Hormozgan province has an area of 70,697 km2 (27,296 sq mi), with Bandar Abbas being its capital. The province has 14 islands located in the Persian Gulf and 1,000 km (620 mi) of coastline. The estimated population of the province, according to the latest census in 2011, is 1,578,183 people, and an estimated 789,712 people live in rural areas. Overall, 384,589 women live in the rural areas of the province. The current study included all the women living in six major rural areas of Hormozgan including Minab, Dehbaz, Bandar-e-Lenge, Qeshm, Bandar-e-Khamir, and Bastak. The total population size and the population of women in these six areas are 179,445 and 86,669, respectively.
We included all the women who referred to healthcare centers of these six areas, within the study period. These women referred to the health care centers to receive vaccination, midwifery, or family planning services. The women were selected consecutively and were included in the survey. The study protocol was approved by the Institutional Review Board (IRB) and the Medical Ethics Committee of Hormozgan University of Medical Sciences. All the participants provided their informed written consents before entering the study.
Study Protocol
All the particpats were interviewed by a trained medical student visiting the healthcare centers for the research project as well as providing healthcare services. All the participants underwent complete pelvic examination in the lithotomy position by the female trained medical student and a midwife. The presence and type of FGM was identified according to the WHO classification and was registered into the data collection forms. The data collection form consisted of several parts including demographic information, knowledge, attitude, and beliefs toward FGM/C. The age at which the FGM was performed was recorded according to the patient’s own or parents’ information. First, participants were asked, “Have you ever been circumcised?” (yes/no). Second, participants were asked, “Do you think this practice should be continued?” (yes/no). Participants who had not heard of FGM/C or female circumcision were also recorded. Our independent variables were basic sociodemographic characteristics such as age, education (illitrate, primary, high school, diploma, MS degree, above), marital status (currently married, single), religion (Shia or Sunni Islam), and nationality (Iranian, Afghan, Arab). We also recorded the family history of FGM/C in mother, sister, and grandmother.
Statistical Analysis
All data were entered into a computer-based data- base and were further analyzed. Statistical package for social sciences (SPSS Inc., Chicago, IL, USA) version 16.0 was used for all statistical analyses. Data are reported as mean ± SD and proportions as appropriate. Parametric data were compared between those undergoing FGM/C and controls using independent t-test, while proportions were compared using chisquared test. A two-sided P value of less than 0.05 was considered as statistically significant.
Results
Overall, we included 780 women who participated in the survey, from the rural areas of Hormozgan. The mean age of the participants was 30.5 ± 14.6 (ranging from 14 to 38) years, and their mean age at which they first had their FMG/C was 5.6 ± 3.6 (ranging from 2 to 38) years. Among the participants, 535 (68.5%) had undergone FGM/C. Thus, the estimated number of the women being circumcised in the area according to screened the population (86,669 people) would be 59,446. In other words, the prevalence was 68,589 in each 100,000 rural female population. The baseline characteristics of the study population are summarized in Table 1. Most participants were married (68.3%) and Iranian (93.1%). The great proportion of the participants were illiterate (36.6%) and had family history of FGM/C. Clitoral nicking was the most common performed procedure (28.7%) followed by type I (clitoridectomy) FGM/C (27.9%).
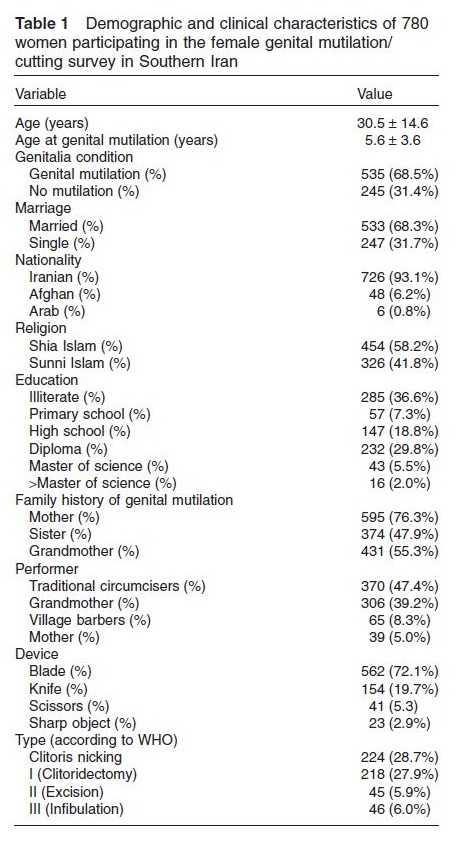 Table 2 demonstrates the determinants of the FGM/C in the study population. Those who have had undergone FGM/C were significantly older (P = 0.002) when compared with controls.
Table 2 demonstrates the determinants of the FGM/C in the study population. Those who have had undergone FGM/C were significantly older (P = 0.002) when compared with controls.
FGM/C was more likely to be performed among Afghans compared with Iranians (P = 0.003) and among married women compared with singles (P < 0.001). FGM/C was associated with Sunni Islam as religion (P = 0.019) and family history of FGM/C in mother (P < 0.001), sister (P < 0.001), and grandmother (P < 0.001). The frequency of illiteracy was significantly higher among those who have had undergone FGM/C compared with controls (P < 0.001). In the same way, the years of education were significantly lower among FGM/C group when compared with controls (4.6 ± 1.3 vs. 9.6 ± 2.6 years; P = 0.013).
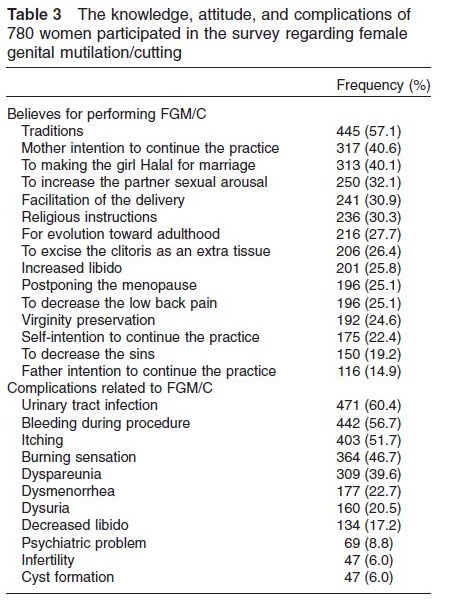
The knowledge and attitude of the participants toward FGM/C and its complications are summarized in Table 3. The most common belief regarding the performance of FGM/C was the ancient traditions of the area (57.1%). Religious instructions were mentioned by 30.3% of the participants, while increasing self-libido (25.8%) and the partners’ sexual arousal (32.1%) were other common causes of performing FGM/C. Mothers had higher intention to continue the practice compared with fathers (40.6% vs. 14.9%; P < 0.001). Overall, 70.6% of those who had undergone FGM/C reported some types of complications (Table 3). UTI was the most common reported complication (60.4%) followed by procedure bleeding (56.7%), itching (51.7%), and burning sensation (46.7%). Also, 8.8% participants reported psychiatric disorders. PTSD was the most common diagnosed mental disorder.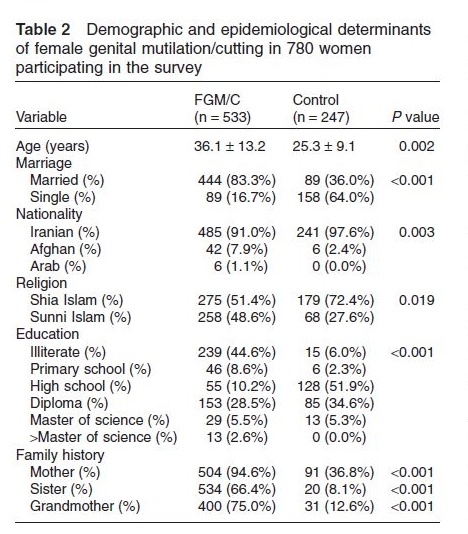
Discussion
FGM/C is a widespread practice being an ancient tradition since antiquity. It persists today primarily in Africa and among small communities in the Middle East and Asia. According to WHO reports, about 100 million women worldwide had undergone FGM/C, while 4 and 5 million procedures are performed annually among female infants and girls [1]. The most severe and invasive subtypes of FGM/C has been reported in Somalian and Sudanese population [15]. Several reports have described the knowledge and attitude as well as epidemiology of the FGM/C in African and Middle East countries. However, data from Iran are scarce. To the best of our knowledge, this is the first study from Southern Iran reporting the prevalence and determinants, as well as knowledge and attitude toward FGM/C. We found that the prevalence of FGM/C was considerably high in Southern Iran despite previous reports [16].
The estimated prevalence of FGM/C varies widely among countries where FGM/C is a routine procedure. This is contrary to the fact that all these countries are geographically neighbors [17]. The differences in epidemiology and characteristics of FGM/C are due to social, historical, traditional, and political variations between countries. More recent studies have demonstrated that nine out of 10 women and girls in Djibouti, Egypt, Guinea, Mali, Northern Sudan, Sierra Leone, and Somalia undergo the procedure annually [12]. It has been also reported that about 87 million girls have undergone the procedure in 27 African countries and Yemen [18]. In the same way, the estimated number of women who have undergone FGM/C was 28,170; 24,710; and 23,240 in Nigeria, Egypt, and Ethiopia, respectively [12,18,19]. We found that 68.5% of all women in Southern rural areas of Iran have undergone some types of FGM/C. Our results are comparable with previous reports from Southern [13] and Northern [14] Iran which showed a prevalence of 70% and 55.7%. This shows that the prevalence of FMG/C is approximately high among rural areas of Iran. The mean age of the participants in the current study was 5.6 ± 3.6 years, which was lower when compared with previous reports from Iran (9.2 ± 14.2 years) [14]. We conclude that the practice is being performed among lower age groups in Southern Iran. The 15- to 19-year age group is considered to be the most common age for FGM/C in most African countries [17,19]. We also found that the prevalence increased by age. Interestingly, we found that some of the girls received FGM after 18 or 21 years of age.
 The age at which FGM is performed varies between countries and even from area to area within the same country; sometimes, it is performed soon after birth and sometimes before marriage [5,6]. We found that the procedure is mostly performed by local circumcisers (47.4%) and grandmothers (39.2%). This is consistent with other studies. Pashaei [14] indicated that the majority of mutilations were performed by traditional midwives and old women (96.4%) who did not use anesthesia (100%). Tag-Eldin et al. [20] also showed that FGM/C among Egyptian women are mostly performed by local circumcisers who do not use local anesthesia. The data of the present study demonstrate that lower educational level is significantly associated with increased prevalence of FGM/C, which is consistent with previous reports from Iran and African countries [14,17,21–23]. The interesting finding of this study was that the FGM/C in southern rural areas of Iran was associated with Sunni Islam as religion. In other words, those with Sunni Islam are more willing to perform the procedure and continue it. Previous reports have shown that FGM/C is associated with Islam as religion [2,16]. Taking all the studies together, it could be concluded that being older, having less education, and being currently or formerly married as opposed to never married is associated with increased odds of having been circumcised. In addition, being Muslim also increases the odds for being circumcised. We have also shown that Sunni Islam is associated with higher prevalence FGM/C when compared with Shia Islam. This could be explained due to higher prevalence of Sunni Muslims in the area. The other explanation is that the Sunni Muslims are more conservative and traditional compared with Shia Muslims in these areas of Iran. It has been also shown that being older, having less education, and being Muslim are associated with higher odds of having had a daughter circumcised [17]. We also demonstrated that positive family history of FGM/C in grandmother, mother, and sister is significantly associated with higher prevalence of FGM/C. Consistent with previous reports, we found that type I FGM/C was the most common performed procedure in the region [1,13,14,17,20,24]. However, clitoral nicking was even more common. This shows that the practice is performed minimized in this region which is limited to nicking and scratching the clitoris.
The age at which FGM is performed varies between countries and even from area to area within the same country; sometimes, it is performed soon after birth and sometimes before marriage [5,6]. We found that the procedure is mostly performed by local circumcisers (47.4%) and grandmothers (39.2%). This is consistent with other studies. Pashaei [14] indicated that the majority of mutilations were performed by traditional midwives and old women (96.4%) who did not use anesthesia (100%). Tag-Eldin et al. [20] also showed that FGM/C among Egyptian women are mostly performed by local circumcisers who do not use local anesthesia. The data of the present study demonstrate that lower educational level is significantly associated with increased prevalence of FGM/C, which is consistent with previous reports from Iran and African countries [14,17,21–23]. The interesting finding of this study was that the FGM/C in southern rural areas of Iran was associated with Sunni Islam as religion. In other words, those with Sunni Islam are more willing to perform the procedure and continue it. Previous reports have shown that FGM/C is associated with Islam as religion [2,16]. Taking all the studies together, it could be concluded that being older, having less education, and being currently or formerly married as opposed to never married is associated with increased odds of having been circumcised. In addition, being Muslim also increases the odds for being circumcised. We have also shown that Sunni Islam is associated with higher prevalence FGM/C when compared with Shia Islam. This could be explained due to higher prevalence of Sunni Muslims in the area. The other explanation is that the Sunni Muslims are more conservative and traditional compared with Shia Muslims in these areas of Iran. It has been also shown that being older, having less education, and being Muslim are associated with higher odds of having had a daughter circumcised [17]. We also demonstrated that positive family history of FGM/C in grandmother, mother, and sister is significantly associated with higher prevalence of FGM/C. Consistent with previous reports, we found that type I FGM/C was the most common performed procedure in the region [1,13,14,17,20,24]. However, clitoral nicking was even more common. This shows that the practice is performed minimized in this region which is limited to nicking and scratching the clitoris.
FGM/C has been associated with several health consequences including long-term and short-term complications [8,25,26]. As many women undergo FGM in infancy, they may not experience any immediate adverse effects. Accordingly, Obermeyer [26] believes that FGM is associated with few number of complications and health consequences and that the hypothesized complications attributed to the FGM/C are not supported by evidence. According to the WHO [11], the immediate complications include infection, urine retention, severe pain, shock, hemorrhage, and death. Long-term consequences of types I and II include abscess, scar neuroma, and the formation of keloid and dermoid cysts. Long-term complications of the type III procedure include those mentioned for types I and II as well as dysmenorrhea, urinary incontinence, and vaginal stenosis. The HIV, hepatitis B, and other blood borne diseases may be transmitted through all forms of FGM [1,11]. As most of our patients were type I, the complications were minimal and limited. Chronic urinary and reproductive tract infections and PID are also linked with FGM. These problems are of particular importance because they are among the leading causes of infertility [8,25]. We also found that UTI and bleeding were the most common reported complications, while cyst formation and infertility were the least common complications. Pashaei [14] demonstrated that circumcised respondents suffered pain (48.2%) and bleeding (1.5%) after FGM. Several studies have showed that women undergoing FGM/C have decreased libido and higher frequency of sexual dysfunction [7,22]. This is considered among the most important mental complications of the procedure [9]. In this study, dyspareunia and decreased libido were reported by 39.6% and 17.2% of participants, respectively. It has also been shown that clitoral reconstruction is associated with improved libido and sexual function [27]. The important point that should be kept in mind is that although there is a global concern regarding HIV transmission via FGM, the direct causal link is still to be identified via large epidemiological studies [28].
We found that the most common reason for performing FGM/C was tradition (57.1%), cleanliness or making the girl Halal (40.1%), and partner’s sexual arousal (32.1%). Religion was mentioned by 30.3% of the participants, while increasing self sexual pleasure was reported by 25.8% of the participants. Pashaei et al. demonstrated that the reasons for FGM/C were tradition and customs (66.7%), cleanliness (17.2%), religion (2.8%), health (2.6%), and control of the sexual desire (1%). It is clear that tradition, religion, and social pressure were the main motives for performing FGM/C. In a study by Tag-Eldin et al. [20], the reasons for FGM were mainly religious (33.9%), cleanliness of the girls (8.9%), and social and cultural traditions (17.9% and 15.9%). Mohammed et al. [23] also reported that among Egyptian women, tradition, cleanliness, and virginity were the most common motives for FGM/C continuation (100%), followed by men’s desire, esthetic factors, marriage, and religion factors (45.2–100%). Our finding is consistent with a previous survey in Iran which showed that FGM/C is a social practice rather than a religious obligation [14]. Generally, there is no reason for FGM/C in Islam. It clear that Islam forbids damaging the human body, and there is no scriptural evidence in the religion to support of FGM/C [19]. The interesting finding was that 40.6% of the mothers mentioned that they would continue the practice for other children. This shows that lack of knowledge contributes to continuation of the practice in the region. More than 80% of the participants also mentioned that their mothers and grandmothers were the main decision makers for this practice. Regarding the role of the mothers and grandmothers in FGM/C, the results are similar to those reported by Tag-Eldin et al. [20] and Herieka and Dhar [29]. Therefore, according to our findings, interventional programs should put emphasis on women’s education on FGM/C hazards.
There were some limitations in our study. The current study was cross-sectional which included the women in the area in order to determine the characteristics of FGM/C in the area. We used a self-reported questionnaire for determining the knowledge and attitude of the participants toward FGM/C. We performed pelvic examination to determine the type of the procedure. This methodology only enables us to report the prevalence of sexual dysfunction among the participants according to their own opinion. Thus, we cannot comment on the association between sexual dysfunction and FGM/C. The other shortcoming of our study is that we did not include the spouses or the fathers of the participants of the study. The role of male partners in continuing the practice is an important issue which is not addressed in the current study. However, this is the first large study on FGM/C in Southern Iran which provides valuable information on characteristics and knowledge toward FGM/C in Iran. Further population interventional studies based on education and media are required to decrease the incidence of FGM/C in the area.
In conclusion, FGM/C is a common practice in rural areas of Southern Iran and is associated with increased age, illiteracy, Sunni Islam religion, Afghan nationality, and positive family history. Lack of knowledge toward FGM/C is the cause of this high prevalence. Increasing the target population knowledge regarding FGM/C via public media and schools would be necessary to cease the continuation of the practice in the region.
download pdf here
Leave a Reply